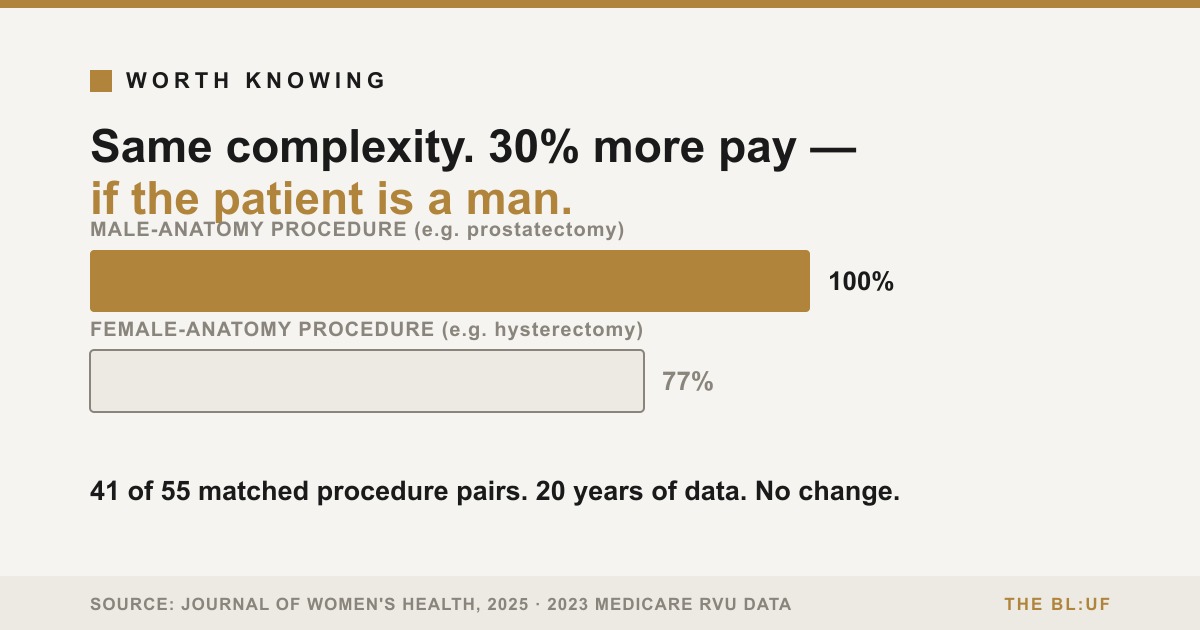
Take two procedures that require roughly the same skill, time, and risk, and differ mainly in whose body is on the table. A hysterectomy and a prostatectomy are both major abdominal or pelvic surgeries, removing an organ, at comparable complexity. Medicare's own relative value system — the formula that determines what a doctor is paid — doesn't see them as equal.
The comparison
A 2025 study in the Journal of Women's Health matched 55 such pairs of gender-specific procedures — verified as anatomically and procedurally comparable by both gynecologists and urologists — against 2023 Medicare data. In 41 of the 55 pairs, three-quarters of them, the procedure performed on female anatomy carried a lower relative value unit (RVU), the number that converts directly into payment. On average, the male-anatomy procedure's RVU was 30% higher. In dollar terms, facility reimbursement averaged 25.6% higher for the male-anatomy procedure — $75.73 more per procedure, on average — and the gap between individual pairs of procedures varied widely.
The same researchers pulled RVU data back to 2003 to check whether the gap has been closing. It hasn't, in any way that reaches statistical significance. Twenty years of the same measurement, the same finding.
It isn't a US-only pattern
A 2023 Canadian study in the Canadian Journal of Surgery ran the same kind of comparison — vulva biopsy against scrotum biopsy, hysterectomy against prostatectomy, ovarian torsion against testicular torsion — against provincial fee schedules instead of Medicare. Same direction, similar size: female-patient procedures reimbursed 26.7% less on average, with 70% of paired procedures showing the gap. (An earlier version of that study reported 28.1%; a letter to the editor pointed out that Yukon has no fee-for-service OB/GYN or urology specialists at all, so including Yukon's published-but-unused fee codes had skewed the number. The authors recalculated and published a correction. The gap got smaller. It didn't go away.)
A second, separate gap
There's a different pattern layered on top of the first one, and it's worth keeping the two apart rather than folding them into one number: female surgeons are paid less than male surgeons for performing the exact same procedure. A study of Medicare payments to neurosurgeons between 2013 and 2020 found male neurosurgeons paid more than female neurosurgeons for the same primary procedure — a gap that held after controlling for practice volume, years in practice, and regional cost differences. A separate, earlier look at ophthalmologists found billing and reimbursement differed by sex too, though that gap was found to trace partly to differences in the volume of charges submitted, not solely to unequal pay for identical work — a real distinction, and one worth not collapsing into the cleaner story.
Put the two mechanisms together and they land hardest on one specialty in particular. Gynecologic surgery has the highest share of female surgeons of any surgical subspecialty, and it's built almost entirely out of procedures on female anatomy — the exact combination that catches both gaps at once. A 2021 commentary in Obstetrics & Gynecology gave it a name: double discrimination.
Why a payment formula matters beyond the paycheck
RVUs aren't set by an insurance company or a government committee working from clinical outcomes data. They're set by the American Medical Association's Relative Value Scale Update Committee — the RUC — whose seats are allocated to national specialty societies, each nominating members to make the case for their own specialty's procedures. The valuations those societies built, decades ago, are still largely the valuations in use today. Twenty years without significant movement isn't evidence that nobody has looked — the Penn et al. trend line runs the full 2003–2023 span and finds the same gap at both ends. It's evidence of a system that isn't built to self-correct.
That matters past the arithmetic of who gets paid what. The 2021 Obstetrics & Gynecology commentary makes the clinical case directly: when gynecologic surgery pays less than comparable-complexity procedures elsewhere, it pushes OB/GYNs toward the better-reimbursed obstetric side of their practice and away from gynecologic surgery — producing more low-volume gynecologic surgeons. Surgical volume and outcomes are linked in the broader literature; a lower-volume surgeon, on average, is a higher-complication-rate surgeon. A reimbursement gap that started as a valuation footnote ends up, several steps downstream, as a patient-safety question.
The pushback, and whether it holds up
The AMA disputes this. Told about findings like these, an AMA spokesperson called claims of inequity between male and female procedures "misinformed," Medscape reported in 2025 — citing, per that account, a 2024 analysis the spokesperson said was conducted jointly by the American College of Obstetricians and Gynecologists and the American Urological Association and found no marked disparity in value. (BL:UF could not independently locate or confirm this analysis — see Receipts.) Part of the argument advanced in that reporting: gynecologic surgery has shifted heavily toward minimally invasive techniques, which are faster and less physically demanding than the open procedures they replaced — and a formula that partly prices work by time and effort will mechanically assign a lower value to a procedure that has gotten quicker, independent of who it's performed on.
That's a real mechanism, not a deflection, and it deserves to be stated plainly rather than waved off. But it doesn't survive contact with the data already matched for exactly this. A 2021 Obstetrics and Gynecology study paired 12 anatomically and technically comparable male- and female-specific procedures using national surgical-outcomes data and measured operative time directly rather than assuming it. The male-specific procedures took longer on average — 136 minutes against 57 — which cuts against efficiency as the explanation, not for it. Female-specific procedures carried a higher RVU-per-hour rate, 10.6 against 9.7. And male procedures still paid more per hour in actual dollars: $599 against $555. Efficiency was already priced in, on both sides of the comparison, and the male-anatomy procedures still came out ahead. In the pair the researchers flagged as its own outlier, radical prostatectomy against hysterectomy, the pattern reversed and the point held anyway: hysterectomy took longer — 168 minutes against 155 — and still paid less per hour, $574 against $601, despite carrying a higher RVU. The study's own conclusion was that the remaining gap traces to which specialty happens to perform the procedure, not to the procedure's own demands.
Two things can be true at once: the AMA's mechanism is real in principle, and it doesn't account for what researchers keep finding when they control for it directly.
What this piece is not saying
This isn't a claim that any individual doctor, insurer employee, or RUC member set out to underpay care for women. The mechanism here is structural and slow-moving — a valuation system last meaningfully reset when the people setting values looked different than medicine does today, left alone for two decades despite repeated measurement showing the same gap. Nothing here says any of the surgeries themselves are performed differently, or that patients are getting worse care in the room. What's being measured is what happens on paper, afterward, when the bill is calculated — and that a formula built once, a long time ago, hasn't been revisited hard enough to close a documented gap that multiple independent teams, in two different countries, keep finding in the same place.
The Receipts
BL:UF doesn't ask you to trust us. Check our work:
Penn M, Colley D, Koirala P, King L, Fitzgerald J. "Price and Prejudice: Reimbursement of Surgical Care on Male Versus Female Anatomies." Journal of Women's Health, published online Feb. 21, 2025. 110 CPT codes / 55 matched gender-specific procedure pairs, verified by gynecologists and urologists, 2023 Medicare data plus a 2003–2023 trend line. DOI: 10.1089/jwh.2024.0984
Chaikof M, Cundiff GW, Mohtashami F, Millman A, Larouche M, Pierce M, Brennand EA, McDermott C. "Surgical sexism in Canada: structural bias in reimbursement of surgical care for women." Canadian Journal of Surgery, Vol 66, Issue 4, July 2023, E341–E347. DOI: 10.1503/cjs.022121. Correction published Vol 66, Issue 6, November 2023, E582 (Yukon data excluded; 28.1% revised to 26.7%).
Gender Differences in Medicare Practice and Payments to Neurosurgeons. JAMA Surgery, 2023. Retrospective cross-sectional study, Medicare data 2013–2020. PMID: 37819669
Reddy AK, Bounds GW, Bakri SJ, Gordon LK, Smith JR, Haller JA, Berrocal AM, Thorne JE. "Medicare Billing and Reimbursement Differ for Women and Men in Ophthalmology." JAMA Ophthalmology, 2017 Mar 1;135(3):205-213.
"Reimbursement for Female-Specific Compared With Male-Specific Procedures Over Time." Obstetrics & Gynecology, December 2021. 12 matched procedure pairs, National Surgical Quality Improvement Program (NSQIP) data, 2015–2018, tracked against 1997 baseline. Measured operative time directly rather than assuming it.
AMA response, via Medscape, "Gynecologic Surgeon Advocates Call for Payment Reform" (2025) — statement from an AMA spokesperson who declined to be identified, and a reference to a 2024 joint ACOG/American Urological Association analysis. Cited via secondary reporting; primary AMA/ACOG/AUA statement not independently obtained.
"Double Discrimination, the Pay Gap in Gynecologic Surgery." Obstetrics & Gynecology (Green Journal), April 2021. Commentary.